When reviewing the primary and long-term efficacy data from the MonumenTAL-1 clinical trial, I was pleased to see the number of patients that experienced responses at 5th line therapy and all being triple-class exposed as well as some patients having prior T-cell redirection therapy. This is why I prefer to prescribe TALVEY® to my adult patients with relapsed or refractory multiple myeloma, and I encourage you to review the efficacy data as you evaluate the needs of your patients, as well.
M. Yair Levy, MD
Texas Oncology-Baylor Charles A. Sammons Cancer Center
Medical Oncologist/Hematologist
Dr M. Yair Levy is a paid consultant for Johnson & Johnson.
MonumenTAL-1 Trial: A Brief Overview
MonumenTAL-1 trial design: The efficacy of TALVEY® as a single agent was evaluated in 219 patients with relapsed or refractory multiple myeloma in the single-arm, open-label, multicenter, phase 1/2 MonumenTAL-1 trial. The trial included patients who had received ≥3 prior systemic therapies, including a proteasome inhibitor, an immunomodulatory agent, and an anti-CD38 monoclonal antibody. Efficacy was based on ORR and DOR as assessed by an IRC using IMWG criteria and reflected patients who had received 4 or more prior lines of therapy.1-3*
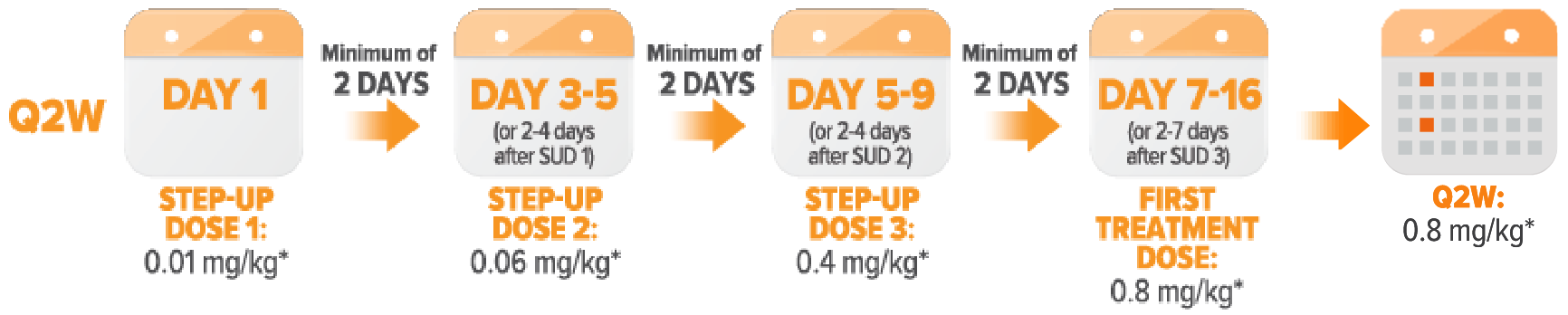
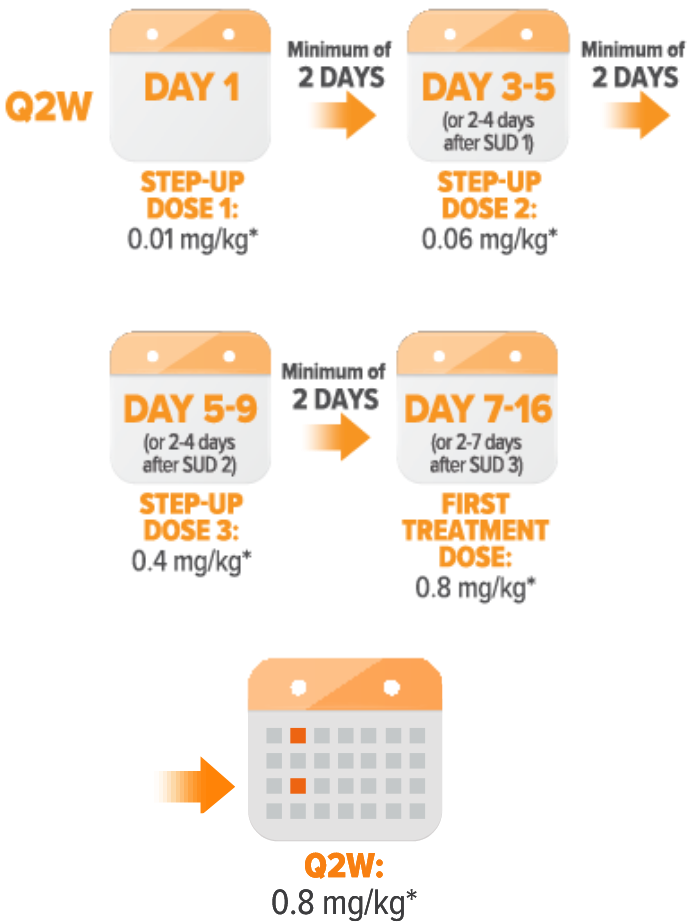
Patients naïve to T-cell redirection therapy† were randomized to receive TALVEY® Q2W or QW:
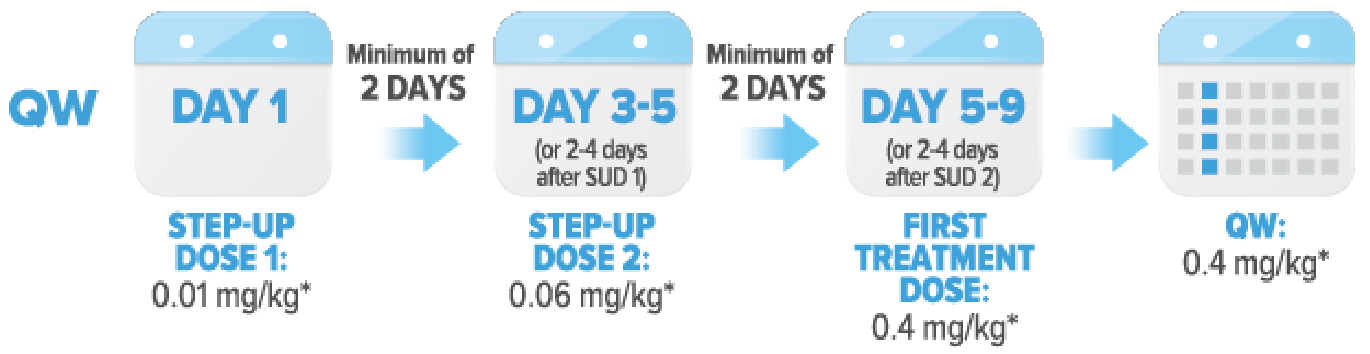
Patients exposed to T-cell redirection therapy† received TALVEY® QW:
Key eligibility criteria1:
- Received ≥3 prior systemic therapies, including a proteasome inhibitor, an immunomodulatory agent, and an anti-CD38 monoclonal antibody
- ECOG PS of 0-2 included
- No T-cell redirection therapy† within 3 months
- No prior Grade 3 or higher CRS related to any T-cell redirection therapy†
- No autologous stem cell transplant within the past 12 weeks
- No stroke, seizure, or allogeneic stem cell transplant within the past 6 months
- No CNS involvement or clinical signs of meningeal involvement of multiple myeloma, or plasma cell leukemia
- No active or documented history of autoimmune disease, with the exception of vitiligo, resolved childhood atopic dermatitis, resolved Graves' Disease that is euthyroid based on clinical and laboratory testing
Primary endpoint: ORR3
Key secondary endpoints: DOR and TTR3
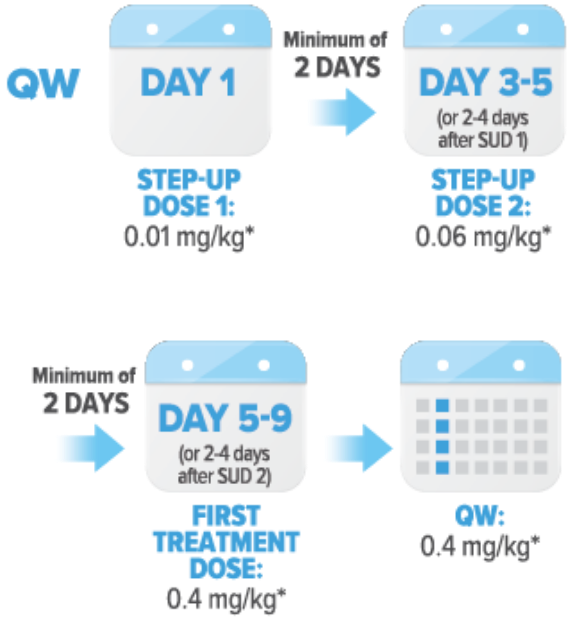
Clinical trial dosing1
Patients received TALVEY® Q2W (0.8 mg/kg) or QW (0.4 mg/kg) as a subcutaneous injection until disease progression or unacceptable toxicity, after the step-up dosing schedule.
Inclusion of patients who were naïve and exposed to T-cell redirection therapy† demonstrated the versatile use of TALVEY®.1
Patients with a range of characteristics, including those with high-risk features, were studied in MonumenTAL-11
In patients naïve to T-cell redirection therapy,† 22% had ISS stage III, 29% had high-risk cytogenetics, 22% had extramedullary disease, and 73% were triple-class refractory

In patients exposed to T-cell redirection therapy,† 81% had prior CAR-T and 25% had prior bispecific antibody therapy

In patients who were triple-class exposed,
TALVEY® provided powerful efficacy1,2
Naïve to T-Cell Redirection Therapy†
73.6% of patients responded to TALVEY®, with over 30% achieving ≥CR1,2

73% of patients responded to TALVEY® monotherapy, with 35% achieving ≥CR1,2

MonumenTAL-1 Longer-Term Follow-Up Analysis: Naïve to T-Cell Redirection Therapy†
You are now viewing a subsequent follow-up analysis of the MonumenTAL-1 trial. This information is not included in the current full Prescribing Information. These long-term follow-up data reflect the patients naïve to T-cell redirection therapy† receiving TALVEY® Q2W; any increase in n-value is due to this longer-term follow-up and additional patients.
Over 70% of patients responded to TALVEY® Q2W dosing, with over 40% achieving ≥CR at a median follow-up of >23 months2,4

73% of patients responded to TALVEY® QW dosing, with 35% achieving ≥CR at a median follow-up of >29 months2,4

Exposed to T-Cell Redirection Therapy†
In patients who were exposed to T-cell redirection therapy,†
Durable responses were seen in patients exposed to T-cell redirection therapy1,2†

MonumenTAL-1 Longer-Term Follow-Up Analysis: Exposed to T-Cell Redirection Therapy†
You are now viewing a subsequent follow-up analysis of the MonumenTAL-1 trial. This information is not included in the current full Prescribing Information. These long-term follow-up data reflect the patients exposed to T-cell redirection therapy† receiving TALVEY® QW; any increase in n-value is due to this longer-term follow-up and additional patients.
72% of patients responded to TALVEY®, with 50% achieving ≥CR§ at a median follow-up of >20 months2,4

Efficacy results reflect patients who received ≥4 prior lines of therapy.1
T-cell redirection therapy refers to both CAR-T and bispecific antibody therapy.1
Baseline cytogenetic data were not available in 11% of patients.
≥CR: sCR+CR.
Reflects the median prior lines of therapy for the entire naïve to T-cell redirection therapy population (Q2W and QW dosing).1
Deep responses: sCR+CR+VGPR.
ORR: sCR+CR+VGPR+PR.
Due to rounding, calculation may not be exact.
≥VGPR: sCR+CR+VGPR
See more clinical study data